Loading Data... |
USING THE WEBSITE
Searching For Results
The results refer to cases operated between 1st July 2014 and 30th June 2018.
Results are published only at individual surgeon level.
Institutional-level data are not published. Hospitals listed are those where BAETS members who have contributed cases operate.
Surgeons may be searched by:
Name (Search by Surgeon):
A drop-down list of contributing members is available, from which an individual can be selected.
Alternatively, if you know the surgeon's name, begin typing in the box, and the list will condense accordingly.
If the name you type is not found, it is likely that the individual is either not a BAETS member, or did not contribute data to the audit during the study period.
Hospital (Search by Hospital):
A drop-down list is available, from which a hospital can be selected.
Alternatively, begin typing a hospital name in the box and the list will condense accordingly.
If the hospital name you type is not found, it is likely that no BAETS members operated there, or that any such members did not contribute data, during the study period. It cannot be inferred that thyroid surgery is not undertaken there.
Address/Postcode:
Either insert a relevant postcode or type in the name of your local town/village. Press 'search by my postcode' and this will load a map showing your location and surrounding hospitals which can be linked to the BAETS audit data. Clicking on the blue hospital icon will link directly to the relevant surgeons' data.
If your local hospital does not appear, it is likely that no BAETS members operated there, or that any such members did not contribute data, during the study period. It cannot be inferred that thyroid surgery is not undertaken there.
Surgeons' Results
Once a surgeon is selected, the following data are presented:
Name
GMC Number
Hospital(s) at which the surgeon operated during the study period.
Dates where cases have been contributed to the audit (so that allowance can be made for e.g. surgeons being newly appointed or retiring from thyroid surgery during the period of study).
Outcomes (accessed by clicking on the 'View Graph' icons):
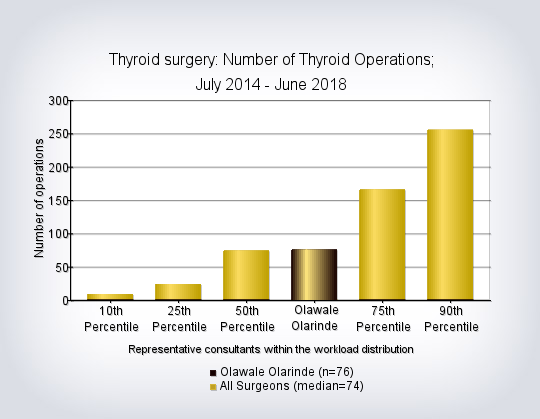
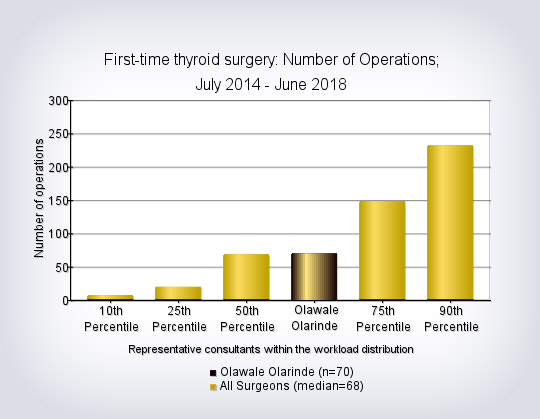
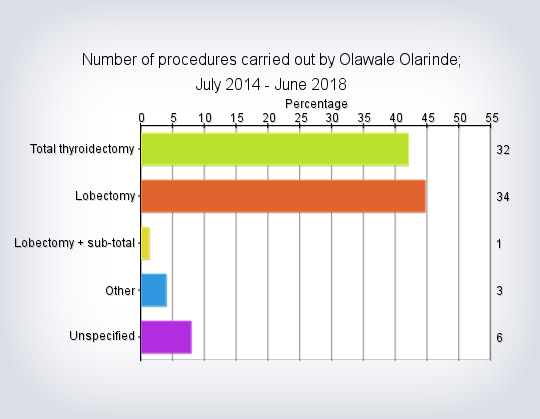
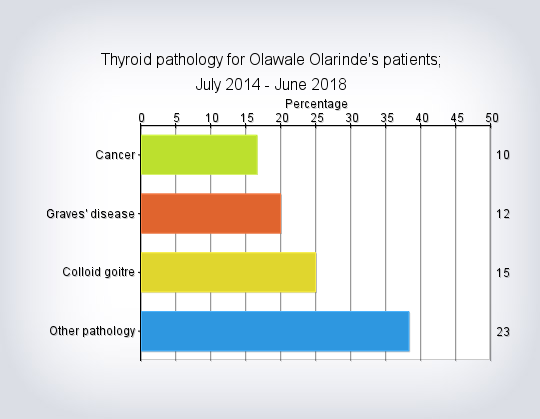
- Case-mix (number of cases, types of operations performed, range of pathology treated)
- Post-operative Length of Stay
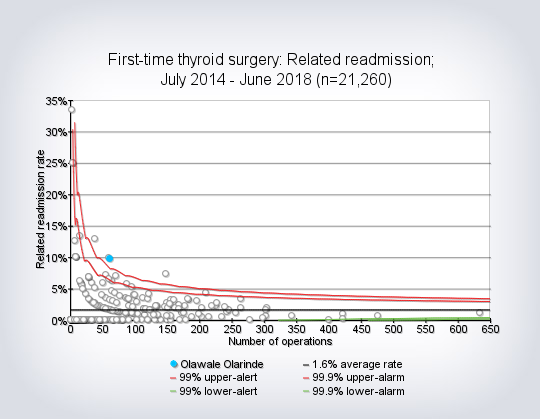
- Re-admission Rate
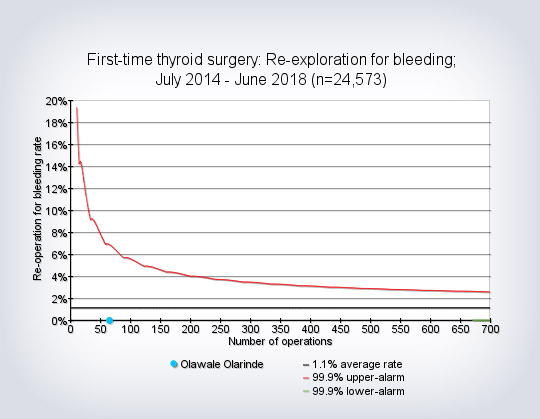
- Rate of Re-exploration for Bleeding
- In-Hospital Mortality
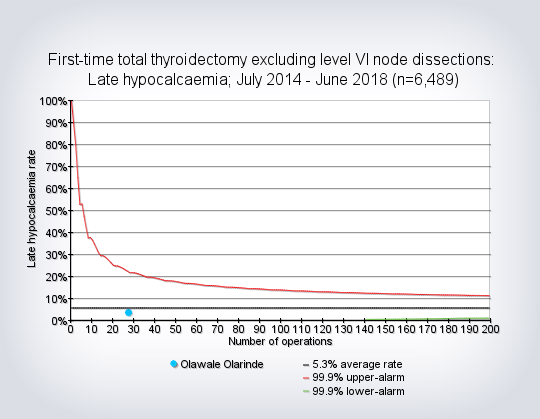
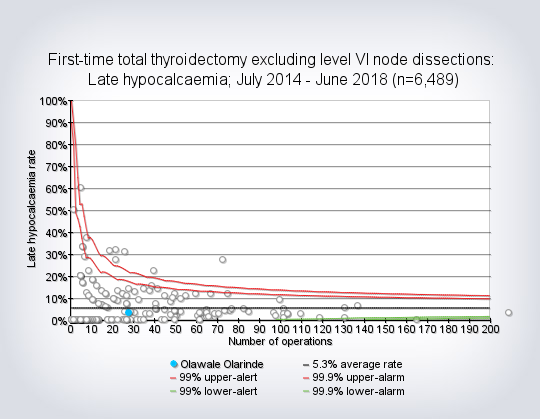
- Late Hypocalcaemia (use of calcium +/- Vitamin D tablets to maintain blood calcium levels at 6 months post-op)
- Vocal cord assessment
- Data Completeness
Results are principally expressed graphically, with accompanying explanatory text.
Complication rates are generally the number of patients having the relevant complication, divided by the total number of cases for that surgeon, so that lower rates usually reflect 'better' results.
In the 'funnel plots', results within the central area (below the red lines and above the green lines) are 'within range' i.e. statistically indistinguishable from the average. Results above the red lines show a significantly higher than expected rate of the complication in question.
Further guidance on the interpretation of funnel plots is included in the following section.
Please also see the Frequently Asked Questions and Glossary links for further information.
Clicking 'Search Again' redirects you to the main Search page.
Guide to Interpretation of Results and Making Comparisons Between Surgeons
Care should be taken in making comparisons between surgeons on the basis of any national audit data, for the following reasons:
A. Data Quality
Any audit relies on the collection, transfer and analysis of information, resulting in a number of potential problems in the quality of the data, including:
- Missing data: where information on a case or outcome has not been entered.
- Inaccurate data: where information has been entered incorrectly.
In the BAETS Audit, responsibility for collection and entry of data onto the audit system rests with the individual surgeon. This may help in ensuring that outcomes are accurately recorded, as there is no reliance on coding of outcomes by third parties, and it is in surgeons' own interests to ensure that results attributed to them are correct. However, it can also contribute to greater levels of missing data, due to limitations or competing priorities on the time allocated to surgeons for such audit activity.
B. Case-mix
With any operation, the risk of certain complications occurring may be affected by features of the patient being operated upon, such as their age or the presence of co-existing illnesses; or by the complexity of the particular operation.
Surgeons taking on more complex cases might therefore be expected to have a higher complication rate, even if their performance is no worse than the average.
For some operations the factors affecting results are well known, and some allowance (or 'risk-adjustment') can be made during analysis, to account for case-mix. In endocrine surgery there are no established mathematical models to make such an allowance. However, previous analyses show that risks of thyroid surgery are higher for:
- Re-operative surgery, compared to First-time surgery (all complications)
- The addition of central compartment (level 6) lymph node dissection to thyroidectomy (in relation to the risk of Late Hypocalcaemia)
For this reason, some outcomes are reported only for first-time surgery and exclude level 6 lymph node dissection. Even in these sub-groups, however, there may be variation in case-mix, contributing to any observed difference in results between different surgeons.
C. Variation in measurement of outcomes
Ascertaining whether or not a complication has occurred is relatively straightforward in some cases e.g. in-hospital mortality, where the outcome is unambiguous and uniformly recorded. For other outcomes, however, this may be complicated by differences in measuring, interpreting and recording the outcome.
This is relevant particularly for 'Late Hypocalcaemia' and 'Vocal cord assessment':
'Late Hypocalcaemia' is currently defined as 'the need for calcium +/- Vitamin D supplements to maintain normal blood calcium levels at 6 months'. This is intended to be a surrogate measure of permanent parathyroid damage.
However:
- Patients may take calcium supplements for reasons unrelated to their surgery e.g. pre-existing vitamin D deficiency or osteoporosis
- Follow-up protocols vary between surgeons
- Opinion varies on whether or not slightly low blood calcium levels require treatment
- Not all patients taking supplements at 6 months will require them indefinitely
For 'Vocal Cord Assessment' other considerations apply:
- There are two main nerves to the voice box, one on each side of the neck, called the recurrent laryngeal nerves. These nerves may be damaged during surgery, which may result in loss of the normal movements of the vocal cords, known as vocal cord palsy. When looking at the rate of vocal cord palsy, allowance must be made for the 'number of recurrent laryngeal nerves at risk'. For instance, during total thyroidectomy the nerves on both sides of the neck are exposed to a risk of injury, whereas during removal of only one lobe of the thyroid (lobectomy), only one nerve is at risk. Surgeons may vary in the proportion of their cases that are total thyroidectomies or lobectomies, which may affect the number of patients with vocal cord palsy.
- Diagnosis of a vocal cord palsy(paralysis of one or other vocal cord) can only be made if the movements of the vocal cords are formally assessed after surgery, usually by fibre-optic laryngoscopy (inspection of the vocal cords with a narrow, flexible telescope via the nose). Some surgeons routinely perform post-operative laryngoscopy on all their cases, while others only do so selectively, perhaps due to vocal symptoms. Some patients may have a vocal cord palsy and yet not notice a significant change in their voice. Therefore, the true rate of vocal cord palsy will be under-estimated by surgeons who do not check the vocal cords routinely after surgery. Conversely, those surgeons who do routinely assess post-operative vocal cord function will naturally have a higher rate of detected vocal cord palsy than those who do so selectively, irrespective of the quality of surgery.
- The timing of the first post-operative vocal cord assessment will also influence this rate (earlier assessments leading to a higher rate, because many vocal cord palsies are temporary). Surgeons vary greatly in this regard, and this information has not, until recently, been recorded in the database.
- The BAETS recommends routine post-operative laryngoscopy. However, not all surgeons have ready access to this investigation, and some patients may decline it. Rates of laryngoscopy may therefore vary between surgeons due to factors beyond their control.
- Vocal cord palsy after thyroidectomy is usually temporary, but can sometimes take several months to recover fully, and sometimes does not recover. If it does not recover, it is deemed 'permanent'. The time interval after surgery beyond which any cord palsy is deemed 'permanent' varies between surgeons, making comparison difficult. Recent updates to the database have addressed this issue, by defining afixed length of follow-up (6 months) for this outcome, but this change occurred after the cases described in this report.
- Some types of thyroid surgery may be more likely to result in a vocal cord palsy e.g. surgery for more advanced cancers or for large goiters extending into the chest. Some surgeons will operate on a greater proportion of these patients than others.
- The rate of missing data for post-operative vocal cord assessment is relatively high. For an uncommon complication such as persistent vocal cord palsy, this makes estimates of outcomes particularly unreliable.
The rate of vocal cord palsy for any surgeon can therefore be affected by the make up of their practice, the proportion of their cases having a post-operative vocal cord check, and at what interval after surgery this is performed, as well as the quality of surgery.
For these reasons, this report concentrates on surgeons' rates of performance of post-operative laryngoscopy and degree of missing data. Data on persistent vocal cord palsy should be considered approximate only, so that comparison between surgeons with respect to this outcome cannot be considered valid at present.
For a more complete analysis of this issue, please see the 4th National BAETS Audit (pages 94-97) report at http://www.baets.org.uk/audit/
D. Random Variation; Interpretation of Funnel Plots
Even when the overall risk of a surgical complication is known, the exact number of complications observed for any one surgeon will be prone to some random variation.
Statistical methods can help identify whether or not the observed variation might be expected by chance alone. Traditionally, 'confidence intervals' are calculated, outlining the limits beyond which chance is less likely to explain the observed variation in outcome. For the purpose of comparing individual surgeons, confidence limits of 99.9% are often used.
For some outcomes, comparison between surgeons can be shown in the form of a 'funnel plot', as in the example below, and this format is used for some of the outcomes reported here. Each surgeon is represented by a 'dot', showing that individual's number of cases and the corresponding percentage of those cases having the complication in question. The black line shows the average complication rate for the whole group of patients (across all surgeons), while the green and red lines show the limits of the confidence intervals, in this example with pre-set values of 99% and 99.9%.
Results within the central funnel (between red and green lines) are considered 'within control limits' i.e. not statistically significantly different from the average.
Results outside the central funnel are very unlikely to have arisen by chance alone, if the surgeon's performance were truly average (0.1% or 1in 1,000).
Other reasons are more likely to explain such results. These might include inaccurate data entry and differences in measuring outcomes, as well as poorer surgical performance.
The example funnel plot below would suggest three individuals whose results are likely to be 'truly' higher than average.

Closing Statement
The BAETS remains committed to using its national audit data to improve the quality of information available on surgical outcomes, and to help contribute to professional development of its membership. This website represents one facet of this process.
Updates at least annually, with additional information on other types of endocrine surgery, are anticipated.
Disclaimer
While every effort has been made to ensure the accuracy of all information contained on this website, Dendrite Clinical Systems Ltd do not accept liability arising from any errors or omissions or the use of or reliance on the information contained in this website and reserve the right to change information and descriptions as and when required.
Surgeon Details:
Olawale Olarinde
-
Casemix
-
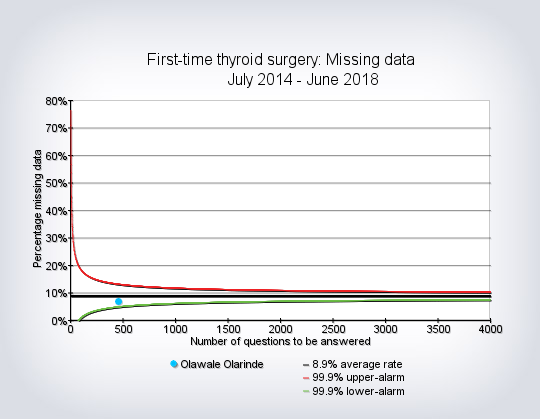
Data Completeness
Extent of missing data on details of Thyroid Surgery or index complications.
Data Completeness
-
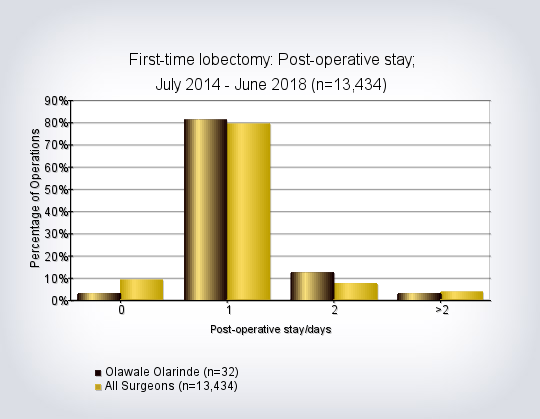
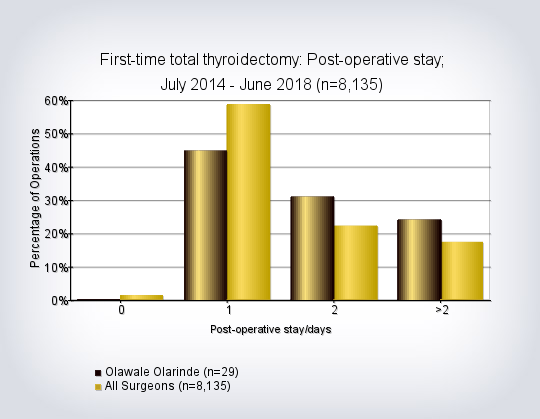
Post-operative Length of Stay
Nights spent in hospital following Thyroid Lobectomy and Total Thyroidectomy.
Post-operative Length of Stay
-
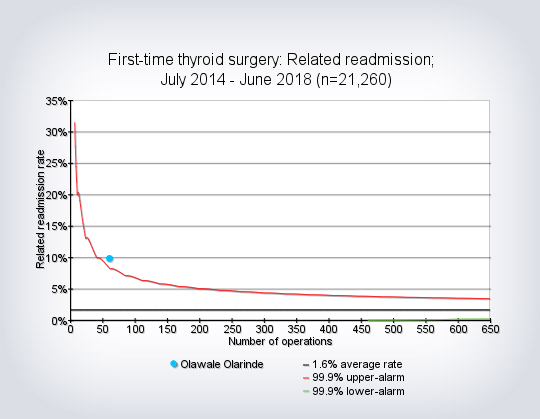
Related Re-admission Rate
Percentage of patients needing re-admission to hospital following Thyroid Surgery.
Related Re-admission Rate
-
Re-exploration for Bleeding Rate
Percentage of patients needing surgery to arrest bleeding following Thyroid Surgery.
Re-exploration for Bleeding Rate
-
In-hospital Mortality Rate
Number of patients dying during the initial admission for Thyroid Surgery.
In-hospital Mortality Rate